In a
very few number of cases (about 13 out of 100), Peyronie's disease goes away
without being treated. Many health care experts suggest treating the disease
without surgery for the first 12 months after the disease is first noticed.
Men
with small plaques, not much curving of the penis, no pain, and no problems
with sex may not need to be treated. If you need to be treated, there are 3
choices.
1
Surgery for Peyronie's Disease: There are 3 basic ways to fix Peyronie's disease with surgery, but
Surgery is not without risks and can include shortening of the penis (scar
retraction) and a chance that the distortion will return. COST:
$25,000 - $35,000
-making
the side of the penis opposite the plaque shorter
Injecting
a drug right into the plaque brings higher doses of the drug to the problem
than when a drug is taken by mouth. Plaque injection is often used for men with
acute phase disease who aren't sure they want to have surgery. The skin is
often numbed before the shot to reduce pain.
Injection
of CCG into collagen-containing structures such as the corpora cavernosa of the
penis may result in damage to those structures and possible injury such as
corporal rupture. Treatment of Peyronie's disease with intralesional therapy:
Injection of collagenase is contraindicated in the treatment of Peyronie’s plaques
that involve the penile urethra due to potential risk to this structure and in
patients with a history of hypersensitivity to collagenase used in any other
therapeutic application or application method. Injection of collagenase
into collagen-containing structures such as the corpora cavernosa of the penis
may result in damage to those structures and possible injury such as corporal
rupture (penile fracture).
Treatment
of Peyronie's disease with penile traction therapy (ANDROPEYRONIE). Penile
traction therapy (PTT) is used to avoid penis shortening after prostate
surgery, which can be used as penile rehab. it would be an effective and safe
method Without expensive risky surgery or injections. Andromedical, a urology
laboratory which has been investigating medical, non-invasive treatments to
Peyronie’s disease, micropenis, post radical prostatectomy penile rehab and
erectile dysfunction for 20 years. Andropeyronie is a simple, effective and
non-invasive treatment of the correction of penile curvature. Andropeyronie
reduces the curvature of the penis + 50%. Andropeyronie increases the length of
the penis and also the girth.
Do you work with men who have
Peyronie’s disease? If so, they might be considering non-surgical treatment
options. One is traction therapy and a recent Journal of Sexual Medicine study
has shown some encouraging results. What is
Traction Therapy?Men
who undergo traction therapy for Peyronie’s disease wear a medical device
specifically designed to gently pull the penis in the opposite direction of the
curve.
A recent study by Spanish researchers found
that this technique had good results for men in the acute stage of Peyronie’s
disease. Fifty-five patients (mean age 50) underwent traction therapy using the
Andropeyronie device, a commonly used brand. A control group of 41 patients
(mean age 48) had no intervention. All of the men had acute-state Peyronie’s
disease. The men receiving traction therapy were instructed to wear the device
for at least six hours a day, but no longer than nine hours. This group also
had penile sonography to evaluate the status of their plaques.
After six months of treatment, the men in
the traction therapy group saw a number of improvements:
· Mean penile curvature at erection was
reduced from 33 degrees at baseline to 15 degrees.
· Mean penile length increased from 12.4
centimeters at baseline to 13.7 centimeters.
· The men reported less pain and improved
erectile function and hardness.
· More men were able to penetrate a partner.
· Sonographic plaques disappeared in 48% of
the patients.
· The need for surgery was reduced in 40% of
the patients. Among the men who did need surgery, about one third were able to
have simpler procedures.
· These results were maintained at a 9-month
follow-up point.
Compliance with treatment was an important
factor for the traction therapy group. The men wore the device for a mean of
4.6 hours a day. However, those who wore it for more than six hours a day generally
had better results. Overall, the researchers concluded that penile traction
therapy “seems an effective treatment” for men in the acute stage of Peyronie’s
disease, as pain, curvature, and sexual function improved in their study group.
Penile traction for Peyronie’s disease treatment ( andropeyronie )
Penile traction for Peyronie’s disease treatment ( andropeyronie ) is a nonsurgical approach that involves the use of a device to straighten the penis by traction therapy ( andropeyronie ). Men who choose penile traction (andropeyronie ) for Peyronie’s disease wear a device for a period of time each day over several months. ( andropeyronie ) is called penis extenders or penile traction devices and are based on the concept that tension from stretching the penis may result in a reduction in penile curvature. Some men without Peyronie’s disease also use penile extenders with the hope they will make their penis longer.
andropenis penis extender penis enlargement
( andropeyronie ) is composed of a plastic ring that fits around the head of the penis and is attached to two movable metal rods that run down the sides of the penis. These rods apply tension upward by placing pressure on a plastic support that rests against the body. Penile traction therapy ( andropeyronie ) can be used both with or without other therapies, including injectable and oral medications.
andropenis penis extender penis enlargement
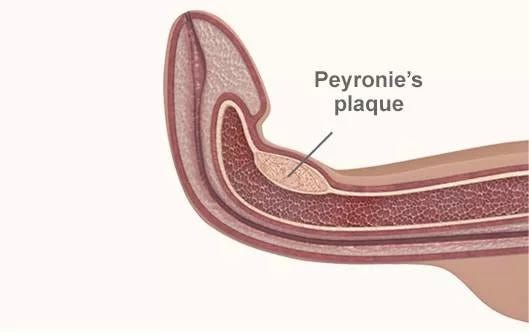
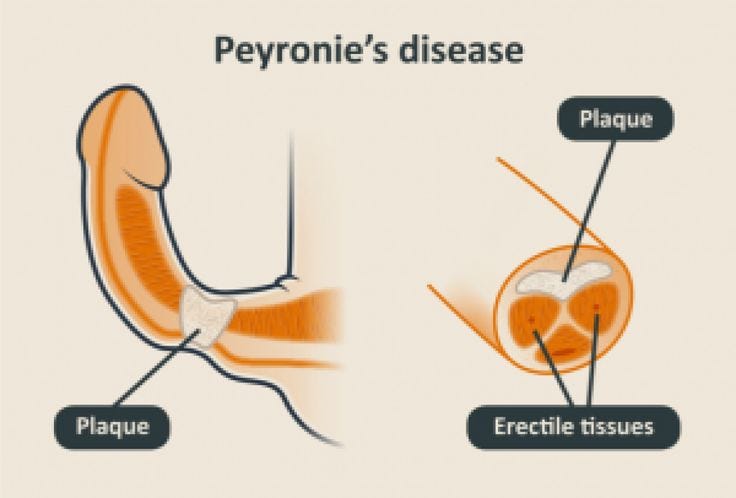
Peyronie’s disease, commonly referred to as curvature of the penis
Peyronie’s disease, commonly referred to as curvature of the penis, is a benign condition. It begins when a dense plaque forms in the outer layers of the penis. The plaque prevents an even expansion during an erection causing a variety of penile deformities during the erect state including curvature, shortening and narrowing.
Peyronie’s disease was initially described by the French surgeon, François Gigot de Lapeyronie, in 1743 even though there are vague references to the disease going back all the way to 1561 and even in sculpture dating back to 3000 BC. Peyronie’s is not a new disease.
Men most often identify Peyronie’s with penile curvature, indentation or other deformities. Deformities associated with Peyronie’s disease may be severe enough to prevent intercourse or, at a minimum, may reduce overall satisfaction. Other symptoms may include inflammation, a lump in the shaft of the penis, pain and erectile dysfunction. As a result, PD can be both physically and psychologically difficult for men and may negatively impact their relationship
Although PD has been recognized and studied for more than 250 years, many misconceptions remain. Common misconceptions include the belief that PD is uncommon, only affects older men, is not associated with ED, lacks treatment options, and resolves over time. None of these statements are true!
Another common and widespread misconception is that men should wait to treat PD until it is at least 6–12 months after the disease has progressed. While this is true for men undergoing surgery, the opposite is true for conservative, less invasive treatments such as traction therapy. A study by Martinez–Salamanca and colleagues clearly demonstrated the benefits with using traction therapy early on in the disease process.
The true prevalence of PD is not known. Depending on the definition of the disease, age, and methods to diagnose, the condition is estimated to affect anywhere from 0.4% to 13% of men. PD is more common in Caucasian men of Northern European origin but can affect men of any heritage. PD may be more common following prostatectomy (16%) or in diabetic men with ED (20%).15–22
Some men are not aware that they have the disease and it is estimated that 15–58% of men may be unaware of the condition.
In 2015, an International Consensus Panel on Sexual Medicine (ICSM) met to discuss the role of penile traction therapy ( ANDROPEYRONIE )in treating various conditions. Based on studies and literature, the panel concluded:
PTT is a viable treatment option to modestly improve penile length
PTT can be used adjunctively before Penile Prosthesis (PP) surgery in men with decreased penile length or after surgery for Peyronie’s disease (PD) to optimize patient outcomes
PTT can correct curvature in men presenting during the acute phase of PD
The benefits of PTT in men with PD in the chronic phase are unclear
How does PD progress?
Peyronie’s disease has two distinct phases characterized by different symptoms. In the early, also called the acute, phase men may experience painful erections, a plaque or bump in the penis, a curved (bent) erection, or a combination of these factors. Not all PD patients experience penile pain or discomfort; however, when present, the pain typically ends 12 to 18 months after the disease starts. In addition, many men notice a decrease in the length of their penis over the first 18 months.
The late or chronic phase begins approximately 6 to 18 months after the first symptoms. During the chronic phase, pain and inflammation typically end and a bend in the penis becomes evident and may worsen. Penile curvature will rarely improve during the late phase of the disease.
Physicians refer to Peyronie’s disease as a sustained or progressive disease. Regardless, the belief that PD will resolve without treatment over time persists. This belief sometimes presents an obstacle to early treatment that may benefit many men.
Does Peyronie’s always result in erectile dysfunction?
Although not all men with Peyronie’s disease will experience worsening erections, in some cases, Peyronie’s can severely deform the penis. This can result in narrowing, buckling or softening of erections. Peyronie’s may also result in painful erections or tenderness at the location of the plaque which may also worsen erections. The misconception that PD is not associated with ED may contribute to a delay in men seeking treatment for the condition. Sometimes patients are misdiagnosed with ED instead of PD. Over half of men reported sexual function worsened over the course of the disease.
Patient characteristics — age and other diseases
Peyronie’s disease can happen to men at any age but is most common among those ages 40–60. It is more common in Caucasians, those who have undergone pelvic surgeries like a prostatectomy, and among those men with certain health conditions such as diabetes
Why does it happen?
The causes of PD are not completely understood but it is believed that it originates from trauma or repeated microtrauma to the erect penis in genetically susceptible men, leading to symptoms such as inflammation, a lump or plaque in the shaft, pain, and deformities of the penis such as curvature.
Are there psychological and psychosocial implications of PD?
PD can cause anxiety, depression, low self-worth, and compromise men’s relationships. Although not much research has been done, it is believed that early identification and treatment of PD may dramatically improve psychological distress particularly for patients who receive timely information and reassurance about the disease and its treatment options
Supplements and vitamins ( ANDROPHARMA CURVATURE )during the initial onset of PD attempt to reduce swelling, pain, and plaque. No oral therapies have been definitively shown to improve the condition, including curvature, penile length or overall disease progression.
Penile injections are often prescribed to treat PD.
Surgery
Surgery is considered the gold-standard therapy for men with PD which has not responded to conservative treatment. To undergo surgery, PD must be stable for at least 6–12 months. The surgical procedure performed depends on several factors including the amount and location of the bend, erectile function prior to PD, patient goals, and surgeon preference. Although surgery corrects curvature in the majority of cases, it may lead to irreversible side effects in some cases including decreased penile length/volume, decreased penile sensation, erectile dysfunction, or recurrence over time. Perhaps because of these side effects, fewer than 30% of men with PD choose to undergo surgery.
Penile traction therapy (PTT) consists of any treatment designed to lengthen or straighten the penis through mechanical forces. PTT is increasingly popular because of its relatively non-invasive nature, low cost, and minimal side effects and the lack of good alternatives to restore lost penile length.
The scientific basis for use of traction therapy is well established. Traction creates mechanical stresses that alter cellular function particularly in cases of fibrosis and, as a result, re-orient collagen fibrils.
A Penis Extender easy to use for Peyronie´s Disease! Reduce Penis Curvature +50%* And pain reduction increase Penis Length +1,5 cm (0.4″) FDA registe
The original ANDROPEYRONIE (20 years) is the only FDA registered and patented PTT penis extender device Manufactured and sold in the US, others traction products are Fakes from China.
Several clinical studies have demonstrated the potential benefits of PTT on curvature correction and restoration of penile length in men with PD. In an early study without a control group, traction improved curvature and length. The study was too small, however, to determine if these findings were due to chance alone.28 In a larger study of men with chronic PD (average duration of 16 months), PTT improved length compare to baseline.29 One study which specifically evaluated men in the acute phase of PD demonstrated significant improvements in penile curvature. Other studies have also shown possible roles for PTT with other conditions including as a primary lengthening therapy, for use prior to penile prosthesis placement, or as a temporary or long-term treatment after PD surgery
In 2015, a consensus panel convened to “summarize the current literature and provide clinical guidelines on penile traction therapy, vacuum erection devices, and penile revascularization.” Consensus panels are convened frequently because “the field of sexual medicine is continuously advancing, with novel outcomes reported on a regular basis. Given the rapid evolution, updated guidelines are essential to inform practicing clinicians on best practices”.
The panel held its meeting during the 2015 International Consultation on Sexual Medicine (ICSM) and the results were published in The Journal of Sexual Medicine in 2016.
Regarding Penile Traction Therapy and based on the literature present at the time of their meeting, the panel made these summary recommendations regarding traction therapy.
Penile traction therapy (PTT) is a viable treatment option to modestly improve penile length (level of evidence (LOE) = 2; strength of recommendation = B; recommended).
Penile traction can be used adjunctively before penile prosthesis (PP) placement in men with decreased penile length or after surgery for Peyronie’s disease (PD) to optimize patient outcomes (level of evidence (LOE) = 3; strength of recommendation = C; Option).
PTT can correct curvature in men presenting during the acute phase of PD (level of evidence (LOE) = 2; strength of recommendation = C; Option).
The benefits of PTT in men with PD in the chronic phase of disease are unclear (LOE) = 3; strength of recommendation = C; Option).
References
[1] Alenghat FJ, Ingber DE. Mechanotransduction: all signals point to cytoskeleton, matrix, and integrins. Science’s STKE : signal transduction knowledge environment. 2002;2002: pe6.
[2] Chung E, De Young L, Solomon M, Brock GB. Peyronie’s disease and mechanotransduction: an in vitro analysis of the cellular changes to Peyronie’s disease in a cell-culture strain system. The journal of sexual medicine. 2013;10: 1259–67.
[3] Laios K, Tsoucalas G, Karamanou M, Androutsos G. Peyronie’s disease in Minoan art. The journal of sexual medicine. 2013;10: 3144–5.
[4] Jalkut M, Gonzalez-Cadavid N, Rajfer J. Peyronie’s disease: A Review. Reviews in urology. 2003;5: 142–8.
[5] Kadioglu A, Tefekli A, Erol B, Oktar T, Tunc M, Tellaloglu S. A retrospective review of 307 men with Peyronie’s disease. The Journal of urology. 2002;168: 1075–9.
[6] Rhoden EL, Riedner CE, Fuchs SC, Ribeiro EP, Halmenschlager G. A cross-sectional study for the analysis of clinical, sexual and laboratory conditions associated to Peyronie’s disease. The journal of sexual medicine. 2010;7: 1529–37.
[7] Kadioglu A, Oktar T, Kandirali E, Kendirci M, Sanli O, Ozsoy C. Incidentally diagnosed Peyronie’s disease in men presenting with erectile dysfunction. International journal of impotence research. 2004;16: 540–3.
[8] Chung E, Yan H, De Young L, Brock GB. Penile Doppler sonographic and clinical characteristics in Peyronie’s disease and/or erectile dysfunction: an analysis of 1500 men with male sexual dysfunction. BJU international. 2012;110: 1201–5.
[9] Smith JF, Walsh TJ, Conti SL, Turek P, Lue T. Risk factors for emotional and relationship problems in Peyronie’s disease. The journal of sexual medicine. 2008;5: 2179–84.
[10] Gelbard M, Lipshultz LI, Tursi J, Smith T, Kaufman G, Levine LA. Phase 2b study of the clinical efficacy and safety of collagenase Clostridium histolyticum in patients with Peyronie disease. The Journal of urology. 2012;187: 2268–74.
[11] Gelbard MK, Dorey F, James K. The natural history of Peyronie’s disease. The Journal of urology. 1990;144: 1376–9.
[12] Nelson CJ, Diblasio C, Kendirci M, Hellstrom W, Guhring P, Mulhall JP. The chronology of depression and distress in men with Peyronie’s disease. The journal of sexual medicine. 2008;5: 1985–90.
[13] Martinez-Salamanca JI, Egui A, Moncada I, et al. Acute phase Peyronie’s disease management with traction device: a nonrandomized prospective controlled trial with ultrasound correlation. The journal of sexual medicine. 2014;11: 506–15.
[14] LaRochelle JC, Levine LA. A Survey of primary-care physicians and urologists regarding Peyronie’s disease. The journal of sexual medicine. 2007;4: 1167–73.
[15] Lindsay MB, Schain DM, Grambsch P, Benson RC, Beard CM, Kurland LT. The incidence of Peyronie’s disease in Rochester, Minnesota, 1950 through 1984. The Journal of urology. 1991;146: 1007–9.
[16] Dibenedetti DB, Nguyen D, Zografos L, Ziemiecki R, Zhou X. A Population-Based Study of Peyronie’s disease: Prevalence and Treatment Patterns in the United States. Advances in urology. 2011;2011: 282503.
[17] Schwarzer U, Sommer F, Klotz T, Braun M, Reifenrath B, Engelmann U. The prevalence of Peyronie’s disease: results of a large survey. BJU international. 2001;88: 727–30.
[18] Rhoden EL, Teloken C, Ting HY, Lucas ML, Teodosio da Ros C, Ary Vargas Souto C. Prevalence of Peyronie’s disease in men over 50-y-old from Southern Brazil. International journal of impotence research. 2001;13: 291–3.
[19] La Pera G, Pescatori ES, Calabrese M, et al. Peyronie’s disease: prevalence and association with cigarette smoking. A multicenter population-based study in men aged 50–69 years. European urology. 2001;40: 525–30.
[20] Mulhall JP, Creech SD, Boorjian SA, et al. Subjective and objective analysis of the prevalence of Peyronie’s disease in a population of men presenting for prostate cancer screening. The Journal of urology. 2004;171: 2350–3.
[21] Tal R, Heck M, Teloken P, Siegrist T, Nelson CJ, Mulhall JP. Peyronie’s disease following radical prostatectomy: incidence and predictors. The journal of sexual medicine. 2010;7: 1254–61.
[22] Arafa M, Eid H, El-Badry A, Ezz-Eldine K, Shamloul R. The prevalence of Peyronie’s disease in diabetic patients with erectile dysfunction. International journal of impotence research. 2007;19: 213–7.
[23] Trost LW, Munarriz R, Wang R, Morey A, Levine L. External Mechanical Devices and Vascular Surgery for Erectile Dysfunction. The journal of sexual medicine. 2016;13: 1579–617.
[24] Mulhall JP, Schiff J, Guhring P. An analysis of the natural history of Peyronie’s disease. The Journal of urology. 2006;175: 2115–8; discussion 18.
[25] Grasso M, Lania C, Blanco S, Limonta G. The natural history of Peyronie’s disease. Archivos espanoles de urologia. 2007;60: 326–31.
[26] Nehra A, Alterowitz R, Culkin DJ, et al. Peyronie’s disease: AUA Guideline. AUA; 2015.
[27] Raheem AA, Garaffa G, Raheem TA, et al. The role of vacuum pump therapy to mechanically straighten the penis in Peyronie’s disease. BJU international. 2010;106: 1178–80.
[28] Levine LA, Newell M, Taylor FL. Penile traction therapy for treatment of Peyronie’s disease: a single-center pilot study. The journal of sexual medicine. 2008;5: 1468–73.
[29] Gontero P, Di Marco M, Giubilei G, et al. Use of penile extender device in the treatment of penile curvature as a result of Peyronie’s disease. Results of a phase II prospective study. The journal of sexual medicine. 2009;6: 558–66.
[30] Nikoobakht M, Shahnazari A, Rezaeidanesh M, Mehrsai A, Pourmand G. Effect of penile-extender device in increasing penile size in men with shortened penis: preliminary results. The journal of sexual medicine. 2011;8: 3188–92.
[31] Nowroozi MR, Amini E, Ayati M, Jamshidian H, Radkhah K, Amini S. Applying extender devices in patients with penile dysmorphophobia: assessment of tolerability, efficacy, and impact on erectile function. The journal of sexual medicine. 2015;12: 1242–7.
[32] Oderda M, Gontero P. Comment on: applying extender devices in patients with penile dysmorphophobia: assessment of tolerability, efficacy, and impact on erectile function. The journal of sexual medicine. 2015;12: 1248.
[33] Levine LA, Rybak J. Traction therapy for men with shortened penis prior to penile prosthesis implantation: a pilot study. The journal of sexual medicine. 2011;8: 2112–7.
[34] Rybak J, Papagiannopoulos D, Levine L. A retrospective comparative study of traction therapy vs. no traction following tunica albuginea plication or partial excision and grafting for Peyronie’s disease: measured lengths and patient perceptions. The journal of sexual medicine. 2012;9: 2396–403.
the Andropeyronie Solution
lieves ANDROMEDICAL provides significant advantages relative to surgery, injections and other conservative therapies including traction devices available today. The table below compares ANDROPENIS to first generation traction systems:
Penile Traction Therapy Summary
Device AndroPenis Physician invented (Peyronie’s specialist) , Opposite force angulation for traction directed at disease site, Optimized Treatment Zone for continuous traction. Returns allowed after use. FDA registered , Designed, made and serviced in USA . Returns in USA.
Improving Men’s Confidence and Sexual Health
OUR MISSION
ANDROMEDICAL was formed in 2000 to meaningfully improve the lives of men with Peyronie’s disease or those with side effects associated with urological surgeries. To achieve this mission, ANDROMEDICAL developed in cooperation with Several Hospitals in USA and Europe.
THE HISTORY AND OPPORTUNITY
ANDROPEYRONIE , the original and patented device with FDA approved was invented by a specialist in Peyronie’s disease (PD) who has treated hundreds of men with PD , with Androcomfort, comfort daily use band.
Andropeyronie’ physician inventor knew traction worked successfully in other areas of medicine such as treating scoliosis or straightening teeth and therefore it could help in treating PD. the devices were designed specifically for PD and offer way to bend the curvature while stretching the penis. Patients were unsure of how much force to apply, and most devices only provided traction intermittently or for the first few minutes of being worn. None of the existing devices were able to provide a consistent and sufficient amount of force to actually improve the underlying disease.
THE GOAL ANDROMEDICAL, in collaboration with hospitals, had several goals for the new device including:
Easy to put on and wear
Require less treatment time and not have to be worn outside the home.
Able to provide opposite angular force to deliver additional stretching to the disease site
THE RESULT
After 20 years of development, testing and collaboration with ANDROMEDICAL , the result is Andropeyronie. The Andropeyronie system provides men with a comfortable, easy to use solution for Peyronie’s disease.
to learn more about ANDROPEYRONIE, the only traction device invented by a Board Certified Urologist specializing in men’s health and Peyronie’s disease.
My Urologist recommended injections and a penile traction device for my recently diagnosed Peyronie’s. I have been very pleased with ANDROPEYRONIE’s ingenious design. The device is compact and easy to use for the recommended one hour per day. The company’s support is unbelievable and staffed by people that are always available and caring. I am very pleased.
Physician and Customer since April, 2018
I’m very pleased with the results of the ANDROPEYRONIE device, and my Peyronie’s has improved significantly since I began using it. I think it will probably turn out to be one of the best purchases I’ve ever made.
Customer since December 2017
The ANDROPEYRONIE is far superior to any of the other devices on the market. It is easy to use and you can actually tell you are getting a good stretching. Although, it has been only a few months, I can see some improvement. If you are thinking about traction you should consider ANDROPEYRONIE.
Customer since November, 2017
The ANDROPEYRONIE traction device appealed to me for several reasons. The main reason being that the device doesn’t have to be worn for several hours a day like others on the market. Its ease of use is also a plus. It’s nice not having to worry about any guesswork in regards to the force of traction being safely and effectively applied while using. Since being diagnosed with Peyronie’s Disease, I lost roughly 2″ in penile length. Since I’ve started traction therapy, I have gained 1.6″ back in length. My experience with the ANDROPEYRONIE device as well as the customer service at ANDROMEDICAL, has been nothing short of great.
Customer since October, 2017
The ANDROPEYRONIE is my third penile traction device and I have to say that it is the iPhone of penis stretchers. I am truly thankful for your work and for letting me know about the device. The amount of force that can be generated is significantly greater than experienced with the other two devices that I purchased in the past.
2019 New Treatment Guidelines for Peyronie's Disease Urological Associations recommends combining the Penile Traction Devices of Andromedical with Collagenase injections to treat Peyronie.
I want to share with you all on how Dr Itua saves my life with his powerful Herbal medicines, I was diagnosed of Oral/Ovarian Cancer which i suffered from for 5 years with no positive treatment until when My son came to me in the hospital when i was laying down on my dying bed waiting for god to call out my name to join him in heaven. My son was so excited that very day he came across Dr Itua on Blogspot, we decided to give him a try although we Americans are so scared to trust Africans but i really have no choice that time to choose life in between so we gave a try to Dr Itua Herbal medicines, god wiling he was a good man with a god gift. Dr Itua send us the herbal medicine it was three bottles. I take it for three weeks instructor and this herbal medicines heal me, cure my Oral/Ovarian Cancer completely I have been living for 9 months now with healthy life no more symptoms. I'm sponsoring Dr Itua in LA Advert on Cancer patent seminar which my son will be participating too and other patent Dr Itua has cured from all kind of human disease, also if you are sick from disease like,Epilepsy,Breast Cancer,Prostate Cancer,Throat cancer,Thyroid Cancer,Uterine cancer,Fibroid,Angiopathy, Ataxia,Arthritis,Brain cancer,Hiv,. Vaginal cancer,Herpes,Colon-Rectal Cancer,Chronic Disease.Amyotrophic Lateral Scoliosis,Brain Tumor,Fibromyalgia,Fluoroquinolone Toxicity,Multiple myeloma,Tach Diseases,Leukemia,Liver cancer, Esophageal cancer,Gallbladder cancer,,Bladder cancer,Gestational trophoblastic disease,Head and neck cancer,Hodgkin lymphoma Intestinal cancer,Kidney cancer,Hpv,Lung cancer,Adrenal cancer.Bile duct cancer,Bone cancer,Melanoma,Mesothelioma,Neuroendocrine tumors Non-Hodgkin lymphoma,Cervical Cancer,Oral cancer,Hepatitis,Skin cancer,Soft tissue sarcoma,Spinal cancer,Pancreatic Cancer, Stomach cancer Testicular cancer, Syndrome Fibrodysplasia Ossificans ProgresSclerosis,Alzheimer's disease,Chronic Diarrhea,Copd,Parkinson,Als,Adrenocortical carcinoma Infectious mononucleosis,Vulvar cancer,Ovarian cancer,,Sinus cancer, Here Is The Wonderful Healer Contact. Name_ Doctor Itua, Email Contact: drituaherbalcenter@gmail.com, Phone/WhatsApp: +2348149277967
I'm here to give my testimony how I was cured from HIV, I contacted my HIV via blade. A friend of my use blade to peel of her finger nails and drop it where she use it, so after she has left i did know what came unto me i looked at my nails, my nails were very long and I took the blade which she just used on her own nails to cut of my finger nails, as i was maintaining my names, i mistakenly injured myself. I did even bother about it, so when I got to the hospital the next week when i was ill the doctor told me that I am HIV positive, i wondered where did i got it from so i remembered how I use my friend blade to cut off my hand so i feel so sad in my heart to the extent that i don’t even know what to do, so one day i was passing through the internet i met a testimony of a lady that all talk about how she was cured by a doctor called DR Imoloa so i quickly emailed the doctor and he also replied to me and told me the requirements which i will provide and I do according to his command, he prepare a herbal medicine for me which I took. He message me the following week that i should go for a test which i did to my own surprise i found that i was HIV negative. He also have cured for all kinds of incurable diseases like: Huntington's disease, back acne, chronic kidney failure, Addison's disease, Chronic Disease, Crohn's Disease, Cystic Fibrosis, Fibromyalgia, Inflammatory Bowel Disease, Fungal Nail Disease, Paralysis, Celia Disease , Lymphoma, Major Depression, Malignant Melanoma, Mania, Melorheostosis, Meniere's Disease, Mucopolysaccharidosis, Multiple Sclerosis, Muscle Dystrophy, Rheumatoid Arthritis, Alzheimer Disease and so many. Thanks to him once more the great doctor that cured me dr. Imoloa so you can also email him via drimolaherbalmademedicine@gmail.com or whatsapp him on +2347081986098. / website- www.drimolaherbalmademedicine.wordpress.com. God Bless you Sir.
PEYRONIE Extender How is Peyronie’s Disease Treated? Andropeyronie is the best option, you do not need dangerous injections of collagenase in the penis How is Peyronie’s Disease Treated? SURGERY - Collagesase - ANDROPEYRONIE In a very few number of cases (about 13 out of 100), Peyronie's disease goes away without being treated. Many health care experts suggest treating the disease without surgery for the first 12 months after the disease is first noticed. Men with small plaques, not much curving of the penis, no pain, and no problems with sex may not need...
Top Penis Extenders — Do These Devices Really Work? HEY! DO NOT Buy Any Product until you read My REVIEW based on Real & Fully Researched Information! Even though most men’s penises are not too small to pleasure their partners, many men still desire something longer. Penile dysmorphophobia is the scientific term for anxiety over the size of your penis. This is common in men throughout the world, especially since the rise of online pornographic videos, where every male star seems to have a freak of nature in their pants. Interesting fact: Although this is still a very unspoken subject, it’s widely believed that the average flaccid length is approximately 3 inches, whereas the erect average length is 5 to 6 inches.For improving the size of your penis without extenders , check out: <img class="progressiveMedia-noscript js-progressiveMedia-inner" src="https://cdn-images-1.medium.com/max/1000/1*ex1HAulFXaXkTILwnEQ5_Q.jpeg"> If yo...













2019 New Treatment Guidelines for Peyronie's Disease
ResponderEliminarUrological Associations recommends combining the Penile Traction Devices of Andromedical with Collagenase injections to treat Peyronie.
I want to share with you all on how Dr Itua saves my life with his powerful Herbal medicines, I was diagnosed of Oral/Ovarian Cancer which i suffered from for 5 years with no positive treatment until when My son came to me in the hospital when i was laying down on my dying bed waiting for god to call out my name to join him in heaven.
ResponderEliminarMy son was so excited that very day he came across Dr Itua on Blogspot, we decided to give him a try although we Americans are so scared to trust Africans but i really have no choice that time to choose life in between so we gave a try to Dr Itua Herbal medicines, god wiling he was a good man with a god gift. Dr Itua send us the herbal medicine it was three bottles. I take it for three weeks instructor and this herbal medicines heal me, cure my Oral/Ovarian Cancer completely I have been living for 9 months now with healthy life no more symptoms.
I'm sponsoring Dr Itua in LA Advert on Cancer patent seminar which my son will be participating too and other patent Dr Itua has cured from all kind of human disease, also if you are sick from disease like,Epilepsy,Breast Cancer,Prostate Cancer,Throat cancer,Thyroid Cancer,Uterine cancer,Fibroid,Angiopathy, Ataxia,Arthritis,Brain cancer,Hiv,. Vaginal cancer,Herpes,Colon-Rectal Cancer,Chronic Disease.Amyotrophic Lateral Scoliosis,Brain Tumor,Fibromyalgia,Fluoroquinolone Toxicity,Multiple myeloma,Tach Diseases,Leukemia,Liver cancer,
Esophageal cancer,Gallbladder cancer,,Bladder cancer,Gestational trophoblastic disease,Head and neck cancer,Hodgkin lymphoma
Intestinal cancer,Kidney cancer,Hpv,Lung cancer,Adrenal cancer.Bile duct cancer,Bone cancer,Melanoma,Mesothelioma,Neuroendocrine tumors
Non-Hodgkin lymphoma,Cervical Cancer,Oral cancer,Hepatitis,Skin cancer,Soft tissue sarcoma,Spinal cancer,Pancreatic Cancer, Stomach cancer
Testicular cancer,
Syndrome Fibrodysplasia Ossificans ProgresSclerosis,Alzheimer's disease,Chronic Diarrhea,Copd,Parkinson,Als,Adrenocortical carcinoma Infectious mononucleosis,Vulvar cancer,Ovarian cancer,,Sinus cancer, Here Is The Wonderful Healer Contact. Name_ Doctor Itua, Email Contact: drituaherbalcenter@gmail.com, Phone/WhatsApp: +2348149277967
I'm here to give my testimony how I was cured from HIV, I contacted my HIV via blade. A friend of my use blade to peel of her finger nails and drop it where she use it, so after she has left i did know what came unto me i looked at my nails, my nails were very long and I took the blade which she just used on her own nails to cut of my finger nails, as i was maintaining my names, i mistakenly injured myself. I did even bother about it, so when I got to the hospital the next week when i was ill the doctor told me that I am HIV positive, i wondered where did i got it from so i remembered how I use my friend blade to cut off my hand so i feel so sad in my heart to the extent that i don’t even know what to do, so one day i was passing through the internet i met a testimony of a lady that all talk about how she was cured by a doctor called DR Imoloa so i quickly emailed the doctor and he also replied to me and told me the requirements which i will provide and I do according to his command, he prepare a herbal medicine for me which I took. He message me the following week that i should go for a test which i did to my own surprise i found that i was HIV negative. He also have cured for all kinds of incurable diseases like: Huntington's disease, back acne, chronic kidney failure, Addison's disease, Chronic Disease, Crohn's Disease, Cystic Fibrosis, Fibromyalgia, Inflammatory Bowel Disease, Fungal Nail Disease, Paralysis, Celia Disease , Lymphoma, Major Depression, Malignant Melanoma, Mania, Melorheostosis, Meniere's Disease, Mucopolysaccharidosis, Multiple Sclerosis, Muscle Dystrophy, Rheumatoid Arthritis, Alzheimer Disease and so many. Thanks to him once more the great doctor that cured me dr. Imoloa so you can also email him via drimolaherbalmademedicine@gmail.com or whatsapp him on +2347081986098. / website- www.drimolaherbalmademedicine.wordpress.com. God Bless you Sir.
ResponderEliminar